Which tachyarrhythmia is shown below?

photo credit: http://www.1393productions.com/wp-content/uploads/2013/10/V-Tach.jpg
Monomorphic Ventricular Tachycardia
Monomorphic Ventricular Tachycardia
- Sustained monomorphic VT - a tachycardia composed of ventricular complexes of a single QRS morphology lasting > 30 seconds
- this may require cardioversion due to hemodynamic compromise
- most ventricular arrhythmias are associated with structural hear disease, typically related to active ischemia or a history of infarct
- scar and the peri-infarct area provide the substrate for re-entry that produces sustained monomorphic V Tach

photo credit: http://www.fammed.wisc.edu/medstudent/pcc/ecg/images/fig41.jpgRight
Bundle Branch Block (RBBB)
Clinical Pearl
Bundle Branch Block (RBBB)
- Right ventricular depolarization is delayed
- Look for R and R' configurations in the chest leads, especially V1 and V2
- this tracing has a classic R and R' configuration in lead V2
Clinical Pearl
- Pulmonary Embolism may cause a RBBB

photo credit: http://withfriendship.com/images/i/43947/left-bundle-branch-block.gif
Left Bundle Branch Block (LBBB)
Left Bundle Branch Block (LBBB)
- The R and R' can be found in the leads V5 and V6 with a LBBB
- Sometimes, the R and R' in V5 or V6 will look like a flattened peak
- V6 in this tracing looks like a flattened peak, while V5 has a more classic R and R' configuration
- also, look for the Q S pattern in lead V1
- the left ventricle depolarizes after the right ventricle

photo credit: http://cdn.lifeinthefastlane.com/wp-content/uploads/2010/04/ECG50641_WPW.jpg
Wolff Parkinson White Syndrome
Wolff Parkinson White Syndrome
- the accessory Bundle of Kent causes ventricular pre-excitation in WPW syndrome
- look for a delta wave, or a slurring of the QRS complex
- the delta wave makes the PR interval look shorter and the QRS complex looks widened
- WPW may cause paroxysmal tachycardia due to rapid conduction of atrial tachyarrhythmias, conduction of automaticity foci in the Kent Bundles, and re-entry
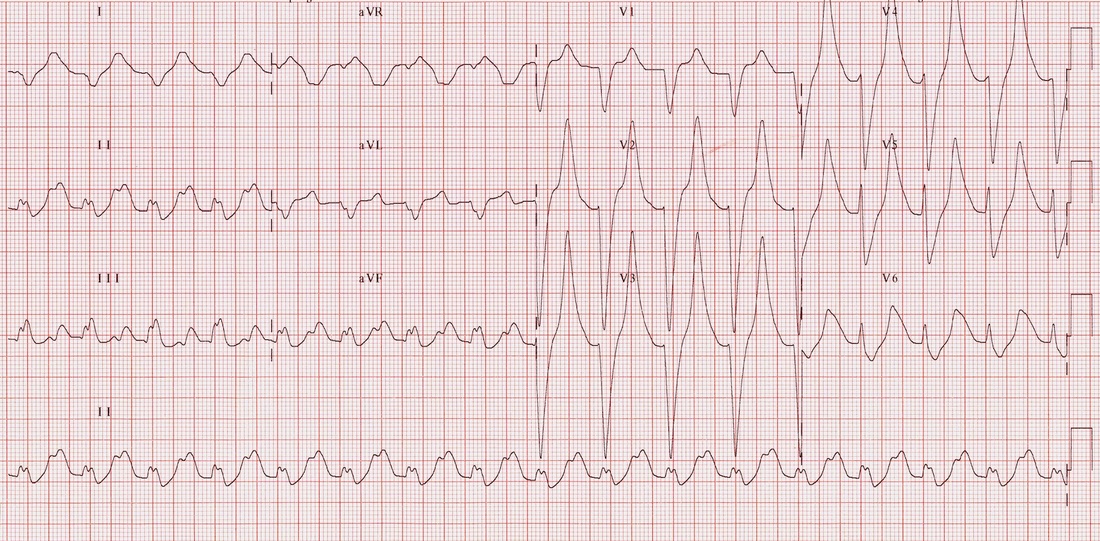
photo credit: http://cdn.lifeinthefastlane.com/wp-content/uploads/2011/02/ECG-Potassium-9.2.jpg
SVT with Hyperkalemia
SVT with Hyperkalemia
- wide QRS complexes that blend with the preceding P wave and the subsequent T wave
- peaked T waves
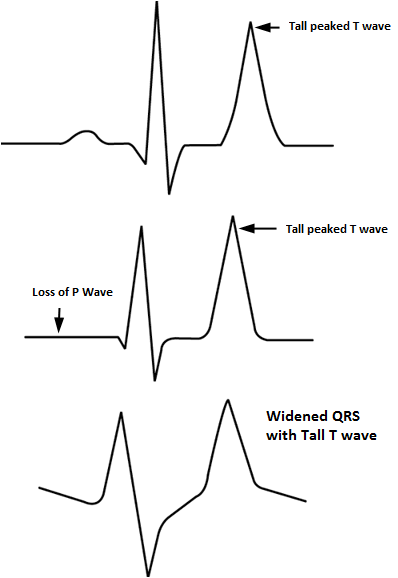
Photo Credit: http://www.aafp.org/afp/2006/0115/afp20060115p283-f1.gif
The effect of potassium on the EKG tracing
What is the treatment?
The effect of potassium on the EKG tracing
- with mild hyperkalemia (serum K+ > 5.5), look for peaked T waves
- with moderate hyperkalemia (serum K+ > 6.0), there will be a loss of the P wave; the P waves dissipate because the atrium is paralyzed by the hyperkalemia
- with severe hyperkalemia (serum K+ > 7.0), there will be a widened QRS with a tall T wave; look for a sinusoidal pattern
What is the treatment?
- calcium chloride or calcium gluconate, glucose and insulin, rescue inhaler, bicarbonate, hemodialysis, and/or kayexylate 15 or 30 grams Q 6 hours
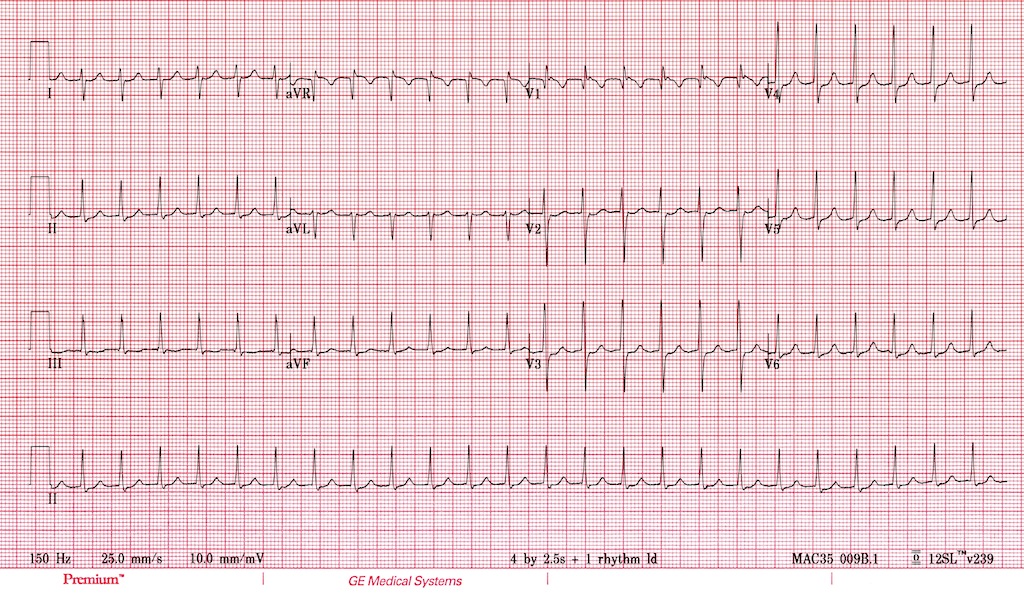
photo credit: http://cdn.lifeinthefastlane.com/wp-content/uploads/2009/09/AVNRT-fast-slow-ppt.jpg
AV Nodal Re-entrant Tachycardia
AV Nodal Re-entrant Tachycardia
- inverted P wave is due to retrograde conduction via the fast pathway that stimulates the atria
- Slow-Fast vs. Fast-Slow vs. Slow-Slow
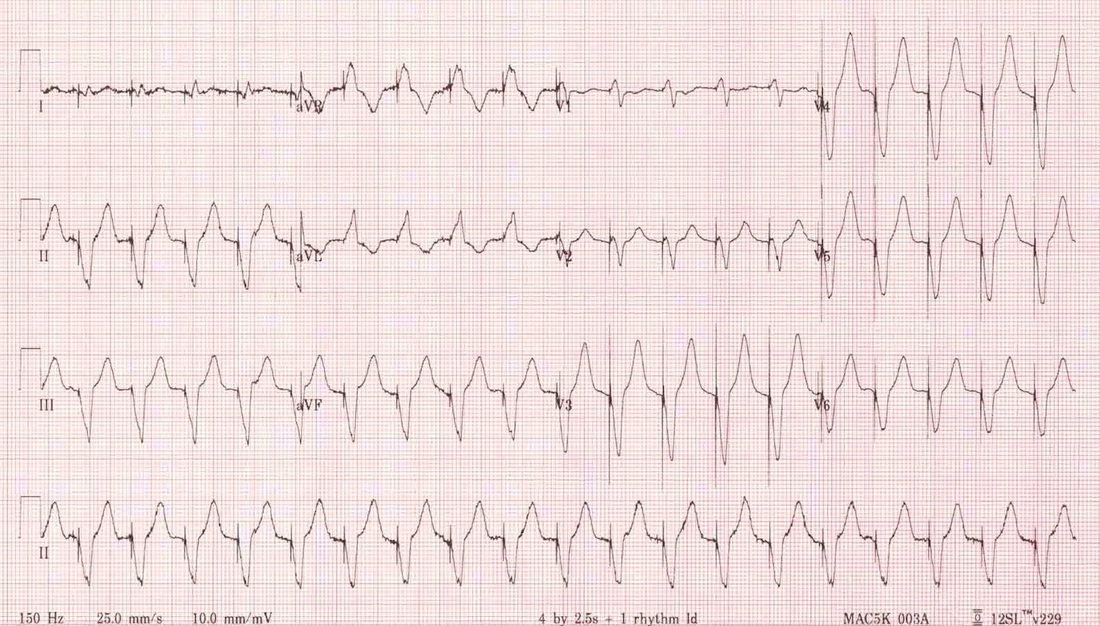
photo credit: http://cdn.lifeinthefastlane.com/wp-content/uploads/2012/01/PMT.jpg
Pacemaker Tachycardia
Pacemaker Tachycardia
- look for electrical activity with each pacemaker impulse
